Prevent leaks!
It’s been big on the news for a while. Nitrous is bad! Say NO (twice) to N2O!
Even the diehard environmentalists don’t want to deny nitrous for labouring women and anxious kids (probably*), so what’s the next best thing to reduce the usage?
Many audits have shown that the vast majority of nitrous is wasted due to leaks within the gas piping (range being 80-100% of total usage).
Simply put, decommissioning nitrous gas pipes and changing to bottled nitrous will be one of the highest yield things you can do for a hospital’s emissions.
In the words of Forbes McGain (Australia’s sustainability hero) it’s not a low hanging fruit. It’s fruit that’s on the ground and rotting.
‘Ok I am keen to do this at my hospital. But where do I start?’
There are many excellent guides out there especially from NHS, and also recently from ANZCA’s blue book in 2025.
I will try to summarise the main points here but the links for further reading are here below..
2025 ANZCA bluebook: https://online.fliphtml5.com/ANZCA1992/rejc/#p=301
Green theatres network: https://greentheatres.online/decommissioning-nitrous-pipelines/
N2O toolkit: https://uclpartners.com/project/nitrous-oxide-toolkit-reducing-waste-in-nhs-trusts/
Solution – Bottled nitrous
The solution is quite simple.
Buy bottled nitrous removing the need for central piping.
Not just in ED, but anaesthetics and obstetrics also.
If this method works in ED, why can’t it work for theatres and obstetrics?
(The answer is of course, it can work).
Then we can decommission the central pipelines.
Removing central gas pipes = smaller bottles = much less risk of mega leaks
What does decommissioning actually mean?
- 1. Deactive N2O alarms of existing network
- 2. Vent the outlets.
- 3. Plug with specially made plugs
- 4. Add labels to all medical gas panels and all outlets plugged
- 5. Disconnect main supply isolate and plug
The good thing is decommissioning can be done by engineering.
We just need to figure out the bottled nitrous system.
Practical points re bottles
But isn’t pressure inaccurate? (It’s good enough)
Most of you probably vaguely remember from the traumatic primary exam, that N2O bottle pressure does not change until all the liquid nitrous evaporates (critical temperature, blah blah 😴), so the bottle needs to be weighed for an accurate gauge of supply.
However once all the liquid is gone the pressure does start to drop giving you an estimate of how much nitrous is left.
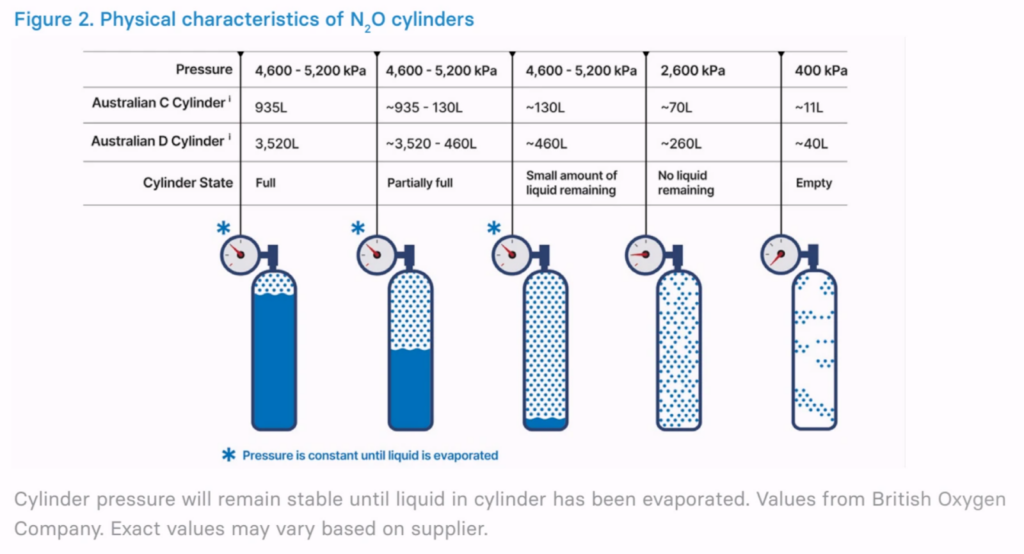
So simply put
- Pressure CANNOT be used to tell you how FULL a cylinder is
- BUT pressure CAN be used to tell you how EMPTY it is
The diagram can be shortened to this for our purposes.
Notice how there’s two pressure point here
- 2600 kPa ≈ 70L C cylinder, 260L D cylinder
- 400 kPa ≈ 11L C, 40L D
Here is my explanation below.
When to replace the cylinder?
Now obviously if we are going to provide a bottle system, we need to know when to replace the bottles reliably.
This will depend on the cylinder size and where it’s connected.
- Commonly used cylinder sizes are
- C (935L)
- D (3520L)
- Connection can be via
- Yoke
or
- Pressure Regulator
(Spoilers – My personal opinion is portable trolley with a Pressure regulator is the best way)
Yoke

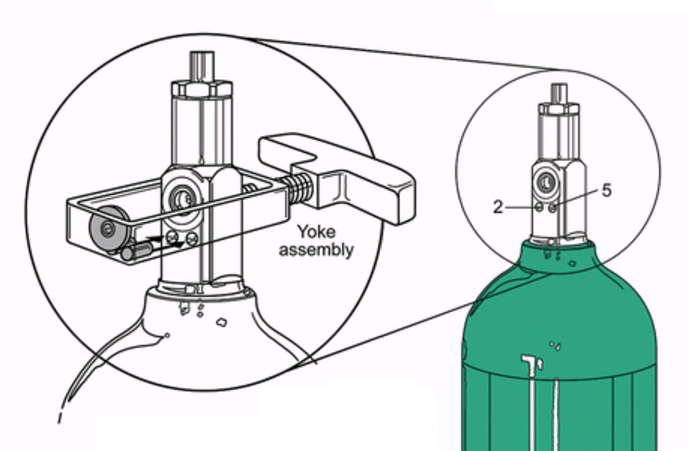
(For the eagle eyed viewer, 2-5 pin index is for oxygen, but you get the idea of a yoke anyway. Hush…)
Yoke (clamp-like device that secures the cylinder to the machine)
- Many anaesthetic machines have an inbuilt yoke allowing cylinders to be fitted to the back of the machine (usually C size cylinders)
- The machine gets the full pressure of the gas bottle (thus measured at the machine), and regulated from there to the circuit
- When connected via yoke, low pressure alarm occurs at 2633kpa for GE machines
- Pressure alarm = 2633 kPa = 70L remaining (in C cylinder)
- This should be plenty of warning time
- 280 minutes of 0.25L/min N2O
- 70 minutes at 2L FGF with 50% N2O (70 min of 1L/min 100% N2O)
- 14 minutes at 10L FGF with 50% N2O (14 min of 5L/min 100% N2O)
Pressure regulator
This is probably the most flexible and cheaper set up, as one portable nitrous trolley system can be implemented to be shared by all theatres rather than buying a cylinder for each theatre (which is in itself important to minimise use. People will only go through the trouble of connecting it if they REALLY felt it was necessary. Just look at what happened with Desflurane use when it was moved out of theatre. Also leaks can happen with bottles too, so less connections involved the better).

D cylinder with pressure regulator
- The pressure regulator is what gets the pressure of the bottle. The pressure is then regulated down to 400kPa from there (ie the machine does not measure the pressure of the bottle)
- Pressure alarm at 254 kPa (GE manual) = 25L remaining
- This should still be sufficient warning time
- 25 minutes of 2L FGF at 50% N2O (= 1L FGF of 100% N2O)
- 5 minutes of 10L FGF at 50% N2O (= 5L FGF of 100% N2O)
Does this setup also work with a C cylinder?
Yes, but a few caveats. Remember the condensed table above?
- If you look at 400kPa, a C cylinder will only have 11L remaining, so a warning 254 kPa is probably not going to be enough of a warning.
However, C cylinders can still be used provided people look at the pressure regulator!
The pressure regulator has a visual indicator with the white line marking the 2600 kPa mark (ie 70L mark for C cylinders).
This means the warning time is the same as calculated in yoke section above.
Pictures of pressure gauges up close below.
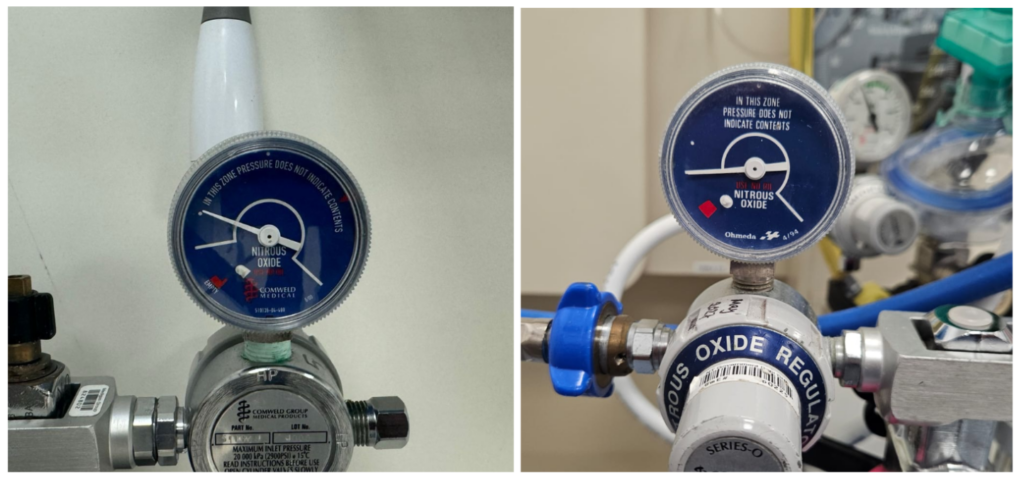
The down side of course is relying on people to check the pressure regulator visually, as there is no audible alarm (But I think if people really wanted to use nitrous, they should educate themselves on this but hey that’s just my opinion).
Now after all that, given it will be 1 bottle for all theatres it would make more sense to use a D cylinder (ie bigger) over a C cylinder for a portable trolley system.
Also when the ‘empty’ bottle is sent back to be refilled, the contents are expelled first resulting in wastage.
As D cylinder can be used until the machine alarm at 254kPa, there will only be 40L left wasted versus the C cylinder at gauge of 2633kPa resulting in 70L of waste.
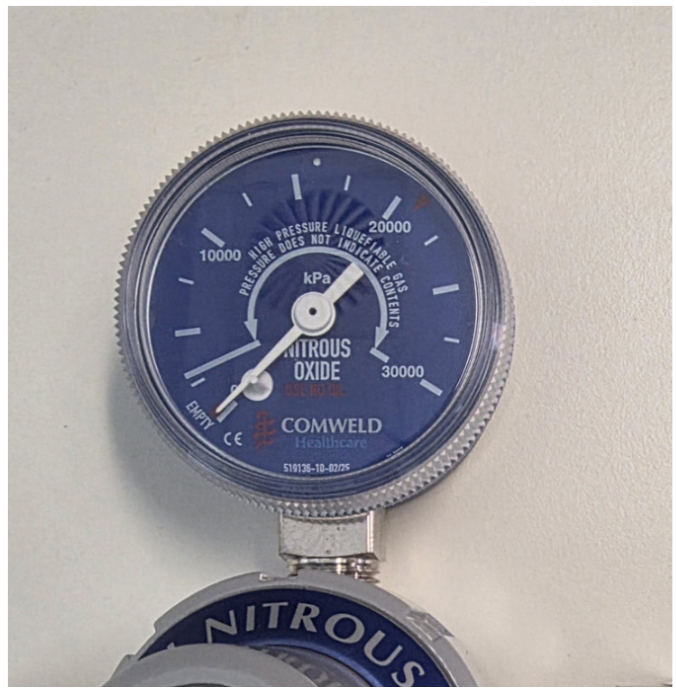
(Variant with the pressures labelled. You can see the ‘pressure does not indicate contents’ stop at ~2600kPa. Although I prefer the much simpler ‘below this white line, you should change the cylinder’ variants). Also this does not have the red indicator.
Storage of N2O cylinders
Be mindful that people can and do abuse N2O cylinders and should be stored in a secure location.
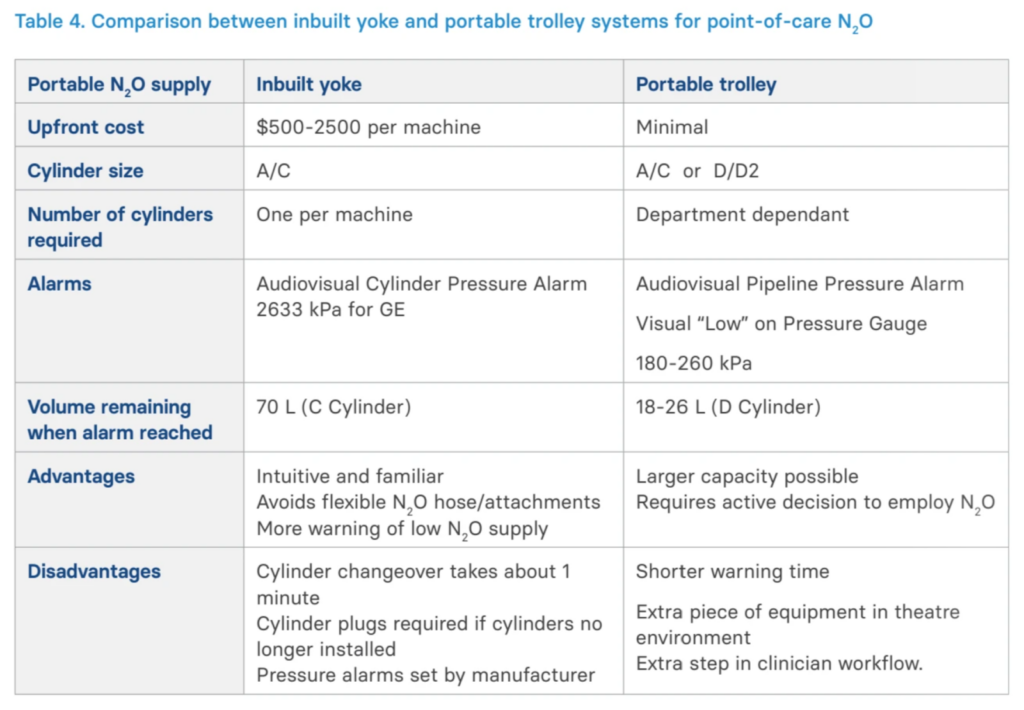
Summary table – Yoke vs Portable trolley
Here is a summary table presented in the blue book including the cost.
Based on this I think a portable trolley system is the winner, but you be the judge for your hospital!
Cost of decommissioning
There is a small cost associated with decommissioning from engineering point of view. This comes from capping the outlets, capping the manifold, and reprogramming the alarm panels.
Here are some real life examples of cost.
300 bed children’s hospital with 120 outlets and one manifold
- Approx $8500 total with labour
- Breakdown
- $32 per outlet (capped)
- ~$80 per manifold (capped)
- Alarm panel reprogramming and commissioning ~ $150 per panel
- Need to be reprogrammed to sensibly not alarm when the nitrous pressure is zero – done by contractors
Prince Charles Hospital (700 beds)
- Total cost $22,800
environmental committee is doing. We did present annual cost savings from environmental initiatives in OT of over $400k – that presentation was after I got the grant but we had presented some other cost savings previously.
The ROI of decommissioning unused wall outlets is easier though: $13.36 service cost per year, decommissioning $50 = ROI 3.6 years.
I also calculated that our leak presents an estimated 5-8 percent of the hospitals scope 1 emissions (based on nitrous being 20% of scope 1 emissions of hospitals in Australia) which obviously is huge savings with one single measure.
$20.300 for decommissioning of the piped system. I’m not sure if they have accounted for all wall outlets though. That’s their problem if they have dodgy maintenance records though
Delivery suite
This may seem like a daunting task, but midwives and also patients are very supportive of the environmental efforts (after all it’s all about the future generations!).
There are a few options to facilitate decommissioning of nitrous in the delivery suite.
1. Use the existing wall blender
Many birthing suites often have a wall blender.
This setup can continue to be utilised with bottles too!
Example of a wall mounted blender

If the midwives are ok to continue the existing wall mounted blenders, this is the simplest option.
Simply have a nitrous bottle with a regulator connected to the wall blender, rather than getting a portable blender.
Advantages
- Uses existing infrastructure – minimal barrier to transition to bottles and minimal education required
- Scavenging available
- Nitrous concentration titration possible
- Cheapest option – only cost is the nitrous bottles
Disadvantage
- Does not provide extra mobility for labouring women (But same as previous)
[NB]
The wall mounted blender shown in the picture may also be able to be changed to a portable blender, but this would require more planning/cost of course.

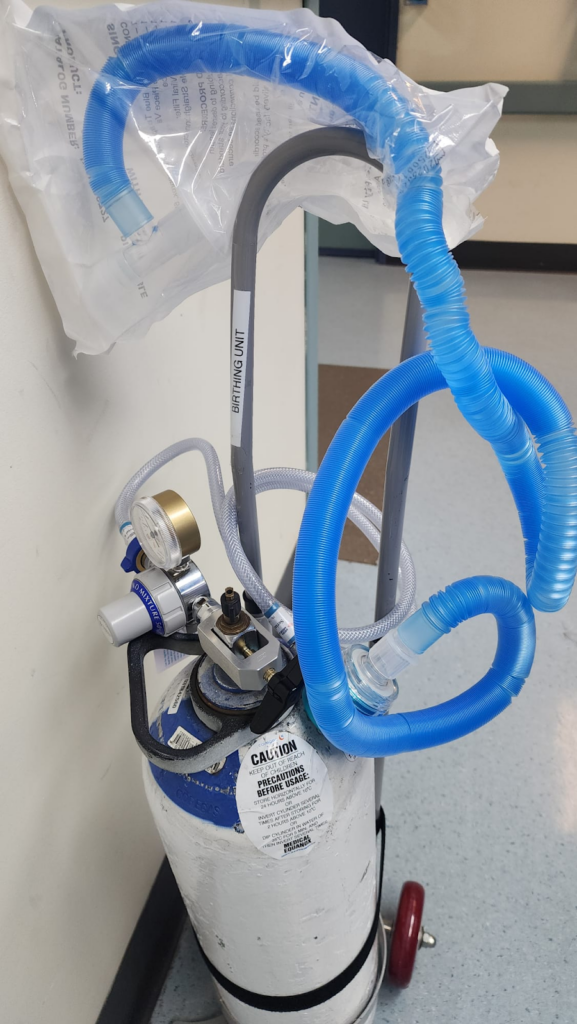
2. Portable entonox
This is a setup that’s fairly common even in places with walled blenders (often used to facilitate mobilisation to the shower).
Entonox

Advantage
- Mobility possible
- Simple – minimal education requirement
- Cheap
- Less environmental foot print vs 75% N2O (5.1kgCO2e/min vs 3.4kgCO2e/min for 50%)
Disadvantage
- No nitrous concentration titration – fixed 50:50 ratio
- No scavenging
[NB]
There aren’t a huge amount of evidence on ideal N2O concentration for labour pain and there is no consensus
- In a study looking at 50%, 60%, 70% N2O in 501 parturients – no significant difference in analgesic efficacy
- A smaller study – Positive association with higher N2O concentration and degree of pain relief
Entonox is widely used in many delivery centres around the world and in the absence of a consensus high concentration should be avoided where possible.
At the National Women’s Hospital in Auckland for example, despite having wall blenders it’s always set at 50% for delivery suite!
3. Portable blenders
There are various blenders available.
Oldest of which uses mechanical blending (which are slowly being phased out) and ‘newest’ blenders are electronically driven.
The real downside is the cost
- Mechanical blenders $~4-5k AUD each – going (or gone) out of fashion

- Electronic blenders $6-13K AUD each
- There are many different brands of electronic nitrous blenders out there
- eAdvantage and Nitronox Plus are two that I am aware of and had enquired about, but I am sure our dentist colleagues can provide more information on different mixers out there


If your hospital has the finance and willpower to utilise portable blenders, electronic blenders will be the best option.
Advantage
- Mobility possible
- Scavenging possible
- Allows titration of nitrous concentration
Disadvantages
- Expensive
- Education required